![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
|
Mycobacterium tuberculosis |
|
Adaptations |
Mycobacterium tuberculosis is a highly successful pathogen because of a number of structural and physiological adaptations. First of all, the bacterium possesses a thick, waxy cell wall that is rich in lipids, many of which are mycolic acids (Figure 1). A similar type of cell wall is observed in the saprophytic bacteria, which are close relatives of M. tuberculosis. Since saprophytic bacteria feed on dead or decaying organic matter and live in a soil environment, a lipid-rich cell wall allows the organisms to resist desiccation. Although M. tuberculosis does not live in the soil but rather within the macrophages of a human or animal host, a high lipid content proves equally important in the survival of the bacterium. When macrophages engulf M. tuberculosis bacilli that are inhaled into the lungs, the macrophages are unable to destroy the bacteria because their lipid-rich cell walls serve as protection. |
|
|
| Figure 1. Transmission electron micrograph of
Mycobacterium tuberculosis bacilli. The lipid-rich cell wall
of M. tuberculosis is a trait shared with the saprophytic
bacteria. |
|
Once inside the macrophages,
M. tuberculosis has the ability to alter the immune response that
would normally take place. After phagocytosis, a macrophage invaginates
its cell membrane around the foreign particle that was just engulfed to
form a vacuole called a phagosome. In phagosome maturation, lysosomes
(organelles that contain enzymes for intracellular digestion) fuse with
the phagosome and release their hydrolytic enzymes. (“Hydrolytic” stems
from the word “hydrolysis,” which refers to chemical reactions that
split compounds with water.) By becoming acidic and hydrolytically
active, the phagosome is then able to digest the foreign particle.
Through mechanisms that are still being questioned, Mycobacterium
tuberculosis can stop phagosome maturation from progressing and thus
maintain the macrophage as a suitable environment in which to live. |
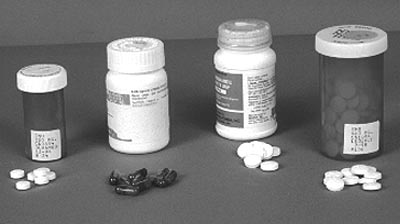 Figure 2. Photograph of four antibiotic drugs used to treat tuberculosis. From left to right: isoniazid, rifampin, pyrazinamide, and ethambutol. |
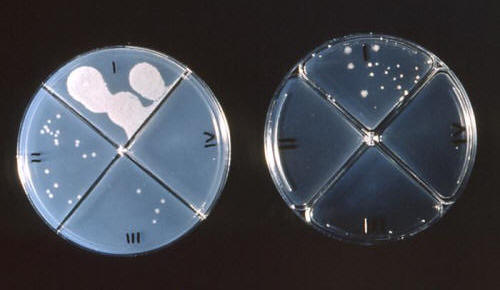
The adaptive ability of Mycobacterium tuberculosis is also evident in cases of antibiotic drug resistance. If a person skin-tests positive for tuberculosis but does not show any signs of disease, he or she is treated for six to nine months with a drug called isoniazid. (See the “Diagnosis” section for more information on tuberculin skin tests.) Cases of active tuberculosis disease require six to nine months on three to four antibiotics, the most popular being isoniazid, ethambutal, rifampin, and pyrazinamide (Figure 2, above). Multiple antibiotics are needed because isoniazid, a mycolic acid inhibitor, kills the rapidly growing bacteria while the other three drugs target slower-growing and dormant bacteria. When individuals fail to comply with antibiotic therapy, either by not taking their medications regularly or by not taking all of the required doses, antibiotic resistance comes into play. In such cases, M. tuberculosis bacilli are exposed to a concentration of antibiotics that is just below the level needed to effectively kill the bacteria. Therefore, the bacteria build up tolerance, making them less sensitive to the effects of the drugs (Figure 3). |
|
|
| Figure 3. Mycobacterium tuberculosis colonies
growing on agar which has been treated with various antibiotic drugs.
Field 1 of the plate on the left represents the control group. |
|
Preventing antibiotics from being activated in the first place is another way in which Mycobacterium tuberculosis can become drug resistant. The enzyme catalase, which the body naturally produces to convert hydrogen peroxide to water and oxygen, also acts on isoniazid, essentially “turning on” the drug. Activated isoniazid works by inhibiting mycolic acid synthesis and, thus, breaking down the cell wall of M. tuberculosis. If the mycobacteria stop the production of catalase, however, isoniazid never gets activated after entering the body. |