![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
|
Mycobacterium tuberculosis |
|
Pathogenesis |
|
|
|
|
|
|
|
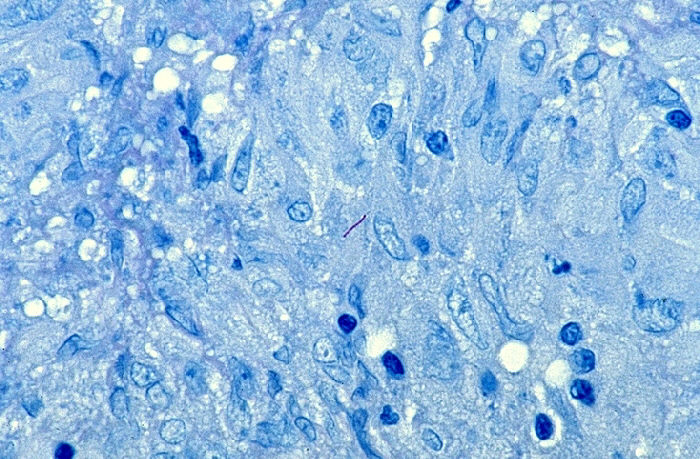
Figure 1. Mycobacterium tuberculosis bacilli visible
within granuloma. This tissue sample was taken from the
endometrial layer of the uterus. This is an example of
tuberculosis disease persisting in an area of the body outside of the
lungs. |
|
|
The interior of a tubercle consists of a gelatinous mass of host cells
and bacilli that gives the damaged tissue a cheese-like consistency.
Therefore, this type of tissue death is referred to as caseation necrosis. If the
immune system is successful in preventing the M. tuberculosis
bacilli from multiplying further, the caseous tubercles become
walled-off and calcified (Figure 2, box 4). Although calcified lesions still contain
viable bacteria, the bacteria cannot be spread to other individuals.
When Mycobacterium tuberculosis lies dormant in the lungs, a
person is said to have a latent tuberculosis infection. Such persons,
who represent 85-95% of infected individuals, show no overt symptoms of
disease. |
|
|
In
5-15% of infected individuals, the immune system fails to prevent the
infection from progressing and the interiors of the caseous lesions become liquefied.
Liquefaction allows viable M. tuberculosis bacilli to spill out
of the tubercles, leaving behind a cavity in the lungs (Figure 2, box 5). When these
bacilli infect lower portions of the lungs or enter the bronchi the
result is an active case of pulmonary tuberculosis disease. People with
pulmonary tuberculosis are capable of spreading the disease to others
through the bacteria in their sputum. They also manifest symptoms such
as weight loss, weakness, night sweats, chest pain, and coughing up
blood. If viable bacilli enter the bloodstream, M. tuberculosis
can travel to organs of the body outside of the lungs (Figure 1, above
and Figure 2, box 3). Known as
extra-pulmonary tuberculosis, this form of the disease is rarely
contagious. |
|
 |
|
|
|
|
|
|
|
|
As mentioned earlier, people with latent tuberculosis infection retain viable M. tuberculosis bacilli within their lungs, even though they are asymptomatic and not infectious. When a person with latent TB becomes immunosuppressed because of old age, lifestyle choices, illness, or a medical condition such as HIV, the dormant bacteria can reactivate within the calcified tubercles. Thus, people with latent tuberculosis infection always run the risk of developing active TB disease. |
|